
From Clinical Trial Breakthroughs to Everyday Practice: A New Horizon in Treating Relapsed Diffuse Large B-Cell Lymphoma
Over the past few years, the treatment landscape for patients with relapsed or refractory diffuse large B-cell lymphoma (R/R DLBCL) has been full of tricky parts and unexpected twists. The recent FDA approval of a triplet regimen that combines brentuximab vedotin (BV), lenalidomide (Len), and rituximab (R) is opening a new chapter for those who have long had limited options, especially patients who are not eligible for stem cell transplant (SCT) or chimeric antigen receptor (CAR) T-cell therapy. As this regimen moves from clinical trials to community practice, it merits an in-depth look at both its promising benefits and the complicated pieces that clinicians and pharmacists must manage.
Understanding the New Combined Therapy for Relapsed DLBCL
The recently approved BV-R2 combination therapy represents an essential shift in the treatment paradigm for R/R DLBCL. Previously, patients who could not undergo SCT or CAR T-cell therapy were confronted with limited and often inadequate alternatives. Now, with the introduction of this new regimen, there is hope for improved overall survival and quality of life—not only for younger patients but also for older adults, who tend to be more affected by such aggressive diseases.
The phase 3 ECHELON-3 trial served as the backbone for this approval. This study compared the triplet regimen (BV, Len, and R) with a regimen that added a placebo to lenalidomide and rituximab. Important metrics such as overall survival (OS), progression-free survival (PFS), and response rates were all significantly better with the novel regimen.
For example, patients on the BV-R2 regimen saw a median OS of 13.8 months compared with 8.5 months with the control, a 37% drop in the risk of death. Similarly, progression-free survival improved by 47%, with a median PFS of 4.2 months versus 2.6 months in the comparison group. With an overall response rate (ORR) of 64% and a complete response (CR) rate of 40%, the results show a durable effect that might very well transform the treatment goals for heavily pretreated patients.
Behind the Scenes: How the Triplet Regimen Works
The BV-R2 therapy is a classic example of how combining different mechanisms of action can produce a synergistic effect. Each medication in the regimen plays a distinct role in fighting the lymphoma, and together these roles complement one another in ways that often defy the challenges posed by complicated pieces of oncology treatment.
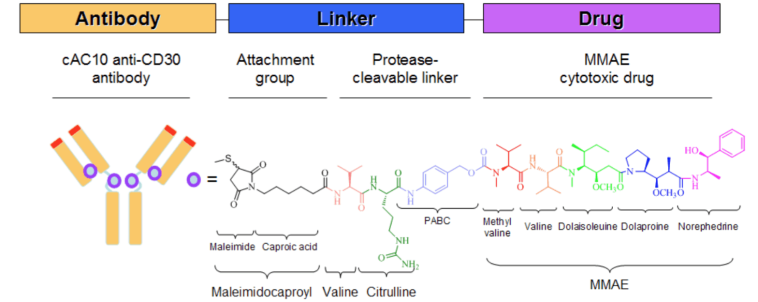
- Brentuximab Vedotin (BV): An antibody-drug conjugate (ADC) that targets CD30 on lymphoma cells, BV is designed to deliver a microtubule-disrupting agent directly to cancerous cells. Its role includes directly inducing cell death and modulating the tumor microenvironment for enhanced immune response.
- Lenalidomide (Len): This immunomodulatory agent boosts the immune system’s ability to fight cancer cells while also promoting antibody-dependent cellular cytotoxicity. It essentially helps the body’s defense system find its path through the maze of malignant cells.
- Rituximab (R): This anti-CD20 monoclonal antibody works by targeting B cells, providing a complementary mechanism to the other two drugs. It has been a staple in treating B-cell lymphomas, reinforcing the overall strategy of the combination.
This powerful combination not only addresses the direct killing of cancer cells but also stimulates a more comprehensive immune response. Even patients with low levels of CD30 expression (less than 1%) have experienced significant benefits, which underscores the regimen’s broad applicability and highlights its potential to get into the nitty-gritty of this challenging disease.
Assessing the Tricky Parts: Safety and Adverse Effects
No breakthrough comes without its own set of tricky parts, and the BV-R2 regimen is no exception. Although the results from the ECHELON-3 trial are promising, the therapy comes with several overlapping adverse effects that require careful monitoring and management.
- Neutropenia: Reported in 43% of patients on the regimen, this low count of neutrophils can lead to an increased risk of infections. Regular blood tests to monitor complete blood counts (CBC) are strongly recommended.
- Thrombocytopenia: With 25% of patients experiencing a drop in platelet counts, there is a risk of bleeding complications that patients and providers need to be wary of.
- Anemia: Present in 22% of cases, anemia might contribute to fatigue and reduced energy, which is especially concerning in older or already frail patients.
Other adverse effects include peripheral neuropathy—a potentially nerve-racking condition due to its cumulative nature—and gastrointestinal issues that can further complicate treatment. These side effects are particularly notable in the months of therapy and can limit treatment duration if not proactively managed. This requires health care professionals to not only be on high alert but also to figure a path for early intervention and supportive care.
Real-World Application: Outpatient Administration and Its Advantages
One of the standout features of the BV-R2 regimen is its outpatient administration. Unlike more invasive and hospitalized therapies such as CAR T-cell therapy—which are off-putting due to their intimidating protocols and the need for close inpatient monitoring—the BV-R2 combination can be delivered in an outpatient setting. This advantage opens up the possibility for wider adoption, especially among patients who prefer or require treatments that do not necessitate lengthy hospital stays.
The shift to an outpatient model means that the therapy is not only more accessible but also likely to be more scalable across various clinical settings. This is key for patients who live in areas with limited access to tertiary care centers. Moreover, the outpatient model reduces many of the nerve-racking financial and logistical issues often associated with inpatient treatments.
Older Adults and Heavily Pretreated Populations: A Closer Look
Older adults, who often face more complicated health profiles, tend to be less tolerant of aggressive treatment protocols. The ECHELON-3 trial’s median patient age was 74, providing vital insights into how the BV-R2 regimen performs in more delicate populations. Even among older adults, the regimen showed a median progression-free survival of 5.7 months compared to 2.8 months in the control group. This age-specific data is particularly important because it suggests that the new combination may help steer through the tricky parts of treating older patients without overwhelming them.
Similarly, patients who have already undergone treatments such as CAR T-cell therapy and bispecific antibodies also witnessed improved outcomes with BV-R2. For instance, the median OS for previously treated CAR T-cell patients improved markedly, underscoring that the regimen brings a new layer of hope and options for those facing repeated relapses. The data indicate that this treatment is not just a fleeting experiment but a robust option for those entangled in a cycle of refractory disease.
Pharmacist Involvement: Critical Roles in Implementation and Patient Safety
A notable aspect of the new BV-R2 therapy is the crucial involvement of pharmacists in its clinical deployment. With their expertise in medication management, pharmacists are pivotally placed to help make a path through the labyrinth of treatment challenges. Their responsibilities span several key areas:
- Patient Selection: Pharmacists must carefully identify which patients are best suited for BV-R2 therapy. This involves evaluating a patient’s treatment history and ensuring they meet the eligibility criteria, specifically those with at least two prior lines of systemic therapy and ineligibility for SCT or CAR T-cell therapy.
- Managing Adverse Effects: By routinely monitoring blood counts and neurological status, pharmacists can detect and mitigate potential adverse reactions early. Given the overlapping toxicities, such as myelosuppression and peripheral neuropathy, timely interventions are crucial.
- Therapeutic Monitoring: Pharmacists also have the responsibility of monitoring treatment responses and ensuring that dosing schedules remain optimal. The close observation of efficacy and side effects allows for prompt dose adjustments when necessary.
- Patient Education: One of the most essential responsibilities, pharmacists can empower patients by explaining both the benefits and potential side effects of the regimen. This educational role is indispensable, as patients who understand their treatment are more likely to adhere to it and alert providers early on to potential complications.
In practical terms, pharmacists serve as a bridge between the patient and the broader healthcare team, ensuring that everyone is aware of how to handle the conflicting bits of this intensive therapy. Their role also extends to providing written guidelines, educational materials, and personalized counsel regarding side-effect management.
Practical Considerations: Outpatient Protocols and Insurance Implications
While the scientific and clinical data are promising, the practical bits surrounding cost, insurance, and general accessibility are equally important. The recommended dose—1.2 mg/kg up to a maximum of 120 mg administered every three weeks—requires robust support systems to help manage patient assessments and follow-ups. The outpatient nature of the regimen is a double-edged sword; although it is more accessible, it also depends heavily on the availability of established protocols that ensure safety and efficacy.
- Resource Allocation: Clinics must have the right resources to supervise blood tests, neurological assessments, and other safety measures that come with BV-R2 therapy.
- Insurance and Cost: Financial aspects remain a challenging twist for many patients. Health care providers and pharmacists must both anticipate and navigate issues related to insurance coverage and out-of-pocket costs, ensuring that the benefits of the new regimen are not limited to those with the best financial resources.
- Training and Standardization: Establishing and adhering to standardized protocols are super important to ensure that all clinical staff understand exactly how to manage the regimen across different practice settings.
A small table to summarize key outpatient administration details can help clarify these requirements:
| Parameter | Details |
|---|---|
| Dosing | 1.2 mg/kg (up to 120 mg) every 3 weeks |
| Monitoring | Complete blood counts, liver studies, neurological assessments |
| Setting | Outpatient infusion center |
| Insurance Considerations | High cost may require prior authorizations; proactive patient support is needed |
These practical considerations can be overwhelming at first glance, but with careful planning and a collaborative approach among oncologists, pharmacists, and support staff, clinics can successfully make the most of the benefits offered by BV-R2.
Tackling Overlapping Adverse Effects: A Shared Responsibility
The overlapping adverse effects associated with the BV-R2 therapy, particularly neutropenia, thrombocytopenia, and anemia, present a shared challenge for the entire healthcare team. Managing these side effects means making your way through a series of nerve-racking monitoring tasks and treatment adjustments. Here are strategies to help manage these complicated pieces:
- Regular Laboratory Monitoring: Routine blood tests are essential to detect any early signs of myelosuppression. Providers must agree on intervals that are both safe and practical, tailoring them to the patient’s overall health status.
- Prophylactic Measures: In some cases, preventive steps such as growth factor support or antibiotics may be needed to mitigate infection risks associated with neutropenia.
- Patient Education and Self-Monitoring: Equipping patients with the knowledge to recognize early symptoms—like fever or unusual fatigue—can lead to faster interventions when necessary.
- Titrating the Dose: In patients who experience severe side effects, adjusting the dose of lenalidomide or temporarily holding the treatment might be required to ensure long-term safety and adherence.
Managing these side effects calls for clear communication and seamless teamwork. Regular meetings between oncologists, pharmacists, and nursing staff can help keep everyone aligned, ensuring that symptoms are addressed before they become overwhelming.
Impact on the Broader Treatment Landscape
The approval of the BV-R2 regimen is significant not just for R/R DLBCL patients but also for reshaping how the broader oncology community approaches treatment for difficult-to-treat hematologic malignancies. Previously, options such as CAR T-cell therapy and bispecific antibodies were not only more costly but also frequently involved a host of intimidating side effects like cytokine release syndrome and neurotoxicity.
By offering a chemotherapy-free, outpatient option that avoids the intense logistics of inpatient care, the new triplet regimen can potentially reduce the overall healthcare burden. It also introduces a level of flexibility that may allow clinicians to better tailor treatment plans to individual patient needs. In turn, this means that patients can expect to have more personalized and manageable treatment experiences.
Yet, the real-world impact of BV-R2 will be largely determined by how well healthcare providers can bridge the gap between clinical trial results and routine practice. This involves not just science but the practical bits—insurance complexities, resource management, and patient education—that ultimately define treatment success.
Emerging Trends: Long-Tail Keywords Worth Focusing On
In today’s rapidly evolving medical field, specific long-tail keywords and topics are garnering extra attention. Here, we take a closer look at several subtopics that complement the discussion around the BV-R2 regimen:
Improved Outcomes in Older DLBCL Patients
For many older patients, treatment options for R/R DLBCL have been limited by both the disease’s severity and the side effects of intensive therapies. The BV-R2 trial has shown that even at an older age, patients can achieve improved progression-free survival and overall survival. These encouraging results help make your way through the previously intimidating treatment protocols that older adults face. This also opens a discussion on tailoring supportive care specifically for an elderly demographic.
Outpatient Cancer Therapies and Patient-Centered Care
A significant advantage of the newly approved regimen is its outpatient administration. This approach benefits patients by reducing hospital stays, allowing individuals to maintain a semblance of normalcy during treatment. Moreover, outpatient care can reduce both direct and indirect costs, making it a super important option in this day and age. Clinics and academic centers alike are now considering how to better support outpatient therapies using robust patient education, home monitoring kits, and telehealth options.
Addressing the Overlapping Issues of Myelosuppression
Any intensive anti-cancer therapy has to contend with the reality of overlapping issues such as myelosuppression—a problem that can complicate other necessary treatments. The strategy to manage these issues involves a clique of measures: frequent monitoring, dose adjustments, supportive care, and effective patient communication. Physicians and pharmacists must figure a path together that mitigates these negative effects without compromising the treatment’s effectiveness.
Insurance Barriers and Resource Allocation for Advanced Lymphoma Therapies
The introduction of advanced therapies invariably brings forward practical challenges, including insurance rejections and resource limitations in community hospitals. Successful implementation of the BV-R2 regime will depend on clear guidelines for documentation, consistent follow-up, and even patient advocacy. End-users, which include physicians and pharmacists, must work with administrative teams to ensure that these barriers are removed, allowing for patient care to be as streamlined as possible.
Looking Ahead: Future Research and Evolving Protocols
The evolution of cancer therapies is an ongoing story, and the FDA approval of BV-R2 is only one chapter in a larger narrative. As more data becomes available and real-world applications accumulate, further refinements in treatment protocols are sure to emerge. Future research might explore:
- The potential for combining BV-R2 with other novel agents
- Optimizing dosing strategies to further reduce severe adverse events
- Understanding long-term outcomes and quality of life improvements in diverse subpopulations
- Examining the economic impact and cost-effectiveness of outpatient versus inpatient treatment models
Each of these areas represents a chance to dig into the small distinctions that make a profound impact on patient care. Moreover, they underscore the notion that while the BV-R2 approval is a remarkable achievement, it also invites further exploration to steer through the fine points of cancer therapeutics in the years ahead.
Final Thoughts: Balancing Promise and Practicality
In summary, the approval of the BV-R2 combination therapy marks a promising but challenging step forward in the realm of R/R DLBCL treatment. On one hand, the improved survival rates, durable responses, and outpatient administration present an exciting new option for patients who have long been left with limited alternatives. On the other hand, the regimen’s overlapping side effects and the practical challenges of outpatient care ask for a high level of vigilance, close monitoring, and effective collaboration between all care providers.
In a landscape where every advancement counts, this approval not only adds a super important tool to the oncologist’s arsenal but also highlights the essential roles that pharmacists and support staff must play. As healthcare professionals, we must work together to manage the tangled issues and subtle parts of this treatment—ensuring that patients receive both the therapeutic benefits and the support they need to manage any adverse effects.
For patients and providers alike, this evolution in therapy is a hopeful sign. It speaks to a future where advancements in science translate into more accessible, manageable, and effective treatments. Whether you are a patient facing the overwhelming burden of R/R DLBCL or a healthcare provider trying to make your way through tricky treatment regimens, the introduction of BV-R2 heralds a new era of possibility and promise.
Ultimately, transformation in cancer care is built not only on robust clinical data but also on the collaborative efforts of multiple stakeholders. By embracing this new outpatient, targeted, and chemotherapy-free option with full awareness of its potential side effects and practical requirements, the medical community can work to ensure that every patient has a fighting chance at improved outcomes and a better quality of life.
In closing, while the transition from clinical trial data to practical, day-to-day implementation is loaded with issues and nerve-racking challenges, it also represents a significant leap toward better care standards. The BV-R2 regimen is an example of innovation that comes with its own set of tangled issues, yet it shows how modern medicine, when supported by well-informed pharmacists and dedicated healthcare teams, can provide workable solutions to some of oncology’s most persistent problems.
As we move forward, it is critical that ongoing research continues and that strategies to address adverse events and logistical obstacles are further refined. Only through continuous collaboration, innovative problem-solving, and patient-centered care can we truly harness the potential of this breakthrough therapy.
Whether you are a seasoned oncologist, a clinical pharmacist, or someone simply interested in the future of cancer care, the journey of BV-R2 from trial results to clinical practice is a vivid reminder that medical progress, although filled with twists and turns, ultimately brings us closer to achieving better outcomes for every patient facing the challenge of R/R DLBCL.
Originally Post From https://www.pharmacytimes.com/view/from-echelon-3-to-clinical-practice-newly-approved-brentuximab-vedotin-with-lenalidomide-and-rituximab-for-r-r-dlbcl
Read more about this topic at
Revolutionizing Cancer Treatment: CAR-NK Cell Therapy …
Revolutionizing Non-Hodgkin Lymphoma Treatment With T …
